
Parental Capacity Evaluations: A Practice Guide for Attorneys and Courts | 2026
By Dr. Lisa Long, Psy.D.
Dr. Long & Associates
Need a Parental Capacity Evaluation?
Virtual evaluations available nationwide — no local evaluator required
This article was originally published as a guide to parental capacity evaluations — what they are, when they are ordered, and what attorneys, caseworkers, and guardians ad litem should expect from the process. It has since become one of the most widely read resources on this topic outside of academic literature — used by attorneys, caseworkers, and guardians ad litem across the country.
In 2026, we substantially expanded this article to address a question we are increasingly asked by referring professionals: how should these evaluations actually be conducted? The sections below now cover both the foundational information from the original article and a detailed explanation of the Parental Capacity Assessment Framework (PCAF) — the structured methodology our practice developed and uses for every parental capacity evaluation we conduct.
What Is a Parental Capacity Evaluation?
A parental capacity evaluation (sometimes called a parental fitness evaluation or parenting assessment) is a forensic psychological evaluation that assesses a parent's ability to meet their child's physical, emotional, and developmental needs. Unlike custody evaluations — which compare two parents to determine the optimal custody arrangement — parental capacity evaluations focus on whether a specific parent can provide minimally adequate care for a specific child.
These evaluations are conducted by forensic psychologists with specialized training in both clinical assessment and the legal system. The evaluation typically includes:
Clinical interviews with the parent being evaluated
Psychological testing to assess personality, mental health, and parenting-related constructs
Review of collateral records including court documents, child protective services records, treatment records, and other relevant documentation
Collateral interviews with individuals who have direct knowledge of the parent's functioning
Parent-child observations when appropriate
The evaluation produces a comprehensive written report that addresses the referral questions and provides the court with empirically-grounded findings to inform legal decision-making.
When Are Parental Capacity Evaluations Ordered?
Parental capacity evaluations serve different functions depending on the legal context. The two primary settings are private family law matters (custody disputes, divorce proceedings) and child welfare proceedings (DSS/CPS cases, termination of parental rights).
Private Family Law Context
In custody litigation, parental capacity evaluations are typically ordered when there are specific concerns about a parent's ability to safely care for the child — concerns that go beyond the normal disagreements between divorcing parents. Common triggers include:
Allegations of abuse or neglect that require expert assessment
Substance abuse concerns where the extent and impact on parenting is disputed
Mental health issues that may affect parenting capacity
Domestic violence history and its implications for child safety
Parental alienation allegations requiring assessment of the parent-child relationship
Reunification planning after a period of limited contact
In private matters, the evaluation is often requested by one party's attorney, ordered by the court on its own motion, or agreed upon by both parties as part of litigation strategy. The evaluator functions as an impartial expert whose role is to assist the trier of fact — not to advocate for either party.
Child Welfare Context
In DSS/CPS proceedings, parental capacity evaluations address different questions with higher stakes. These evaluations typically occur when:
Reunification is being considered after a child has been removed from the home
Termination of parental rights (TPR) is being contemplated and the court needs expert opinion on the parent's capacity and prognosis for change
Case planning decisions require assessment of what services might address identified deficits
Permanency hearings need empirical grounding for decisions about the child's future
In child welfare contexts, the central question often extends beyond current capacity to include capacity to change — can this parent, with appropriate services and within a reasonable timeframe, develop the skills and functioning necessary to safely parent this child?
The sections above describe what parental capacity evaluations are and when courts order them. What they do not address — and what the field itself has largely failed to address — is how these evaluations should be conducted. The remainder of this article turns to that question: the methodological challenges that make parenting capacity one of the most difficult forensic assessments to do well, the structural gap in the field's available tools, and the framework our practice built to close it.
The Structural Problem
Whether you are a family law attorney, a DSS caseworker, or a guardian ad litem, you have likely received parental capacity evaluations that left fundamental questions unanswered. Reports that document a parent's depression or substance use disorder but never establish whether those conditions actually impair their ability to care for their child. Forty-page documents that catalog clinical findings without ever arriving at a clear answer to the question the court asked.
The problem is not simply individual evaluator quality. It is a structural gap in the field itself: there is no empirically-validated, standardized assessment instrument for parenting capacity.
Consider what exists in other forensic domains. Violence risk has the HCR-20. Sexual offense recidivism has the Static-99 and STABLE-2007. Psychopathy assessment has the PCL-R. Competency to stand trial has the MacCAT-CA. Each of these domains developed structured tools that organize clinical judgment around empirically supported factors, constrain subjectivity, and produce defensible conclusions. Parenting capacity assessment has no equivalent.
This is not a new observation. The field has produced important conceptual and clinical contributions over the past four decades:
Thomas Grisso's Functional Model (1986) established that forensic assessments should focus on specific functional capabilities rather than diagnostic categories — a principle that remains the central critique of poor-quality parenting evaluations, and one the field still routinely violates.
Sandra Azar's Functional-Contextual Approach (1998) applied Grisso's framework specifically to parenting, challenging the assumption that psychiatric diagnosis predicts parenting inadequacy and emphasizing that parenting must be assessed in context — considering environmental factors and the specific demands of individual children.
Karen Budd's Clinical Practice Model (2001, 2005) provided the most comprehensive guidance for parenting evaluations in child protection contexts, articulating three core features: center the assessment on parenting rather than general adult functioning, employ a functional approach emphasizing behaviors and skills in everyday performance, and apply a minimal parenting standard rather than comparing parents to optimal functioning. Her concept of "parent-child fit" — assessing whether this parent's capacities match this child's specific needs — became foundational.
The UK Framework for Assessment (2000) organized parenting capacity into six dimensions: basic care, ensuring safety, emotional warmth, stimulation, guidance and boundaries, and stability. This framework provided structured domains for social work assessment but was designed for ongoing case management, not forensic evaluation.
The Capacity-to-Change Literature (Harnett 2007; Platt & Riches 2016) recognized that parenting capacity at a single point in time is insufficient for permanency planning. Courts need to know not just where parents are, but whether they can get where they need to be. UK researchers developed protocols for assessing willingness and ability to make sustained behavioral change — conceptually distinct from current parenting abilities.
Each of these contributions advanced the field. None solved the fundamental problem.
Grisso and Azar provided methodology but not operational content — they told evaluators how to think but not what to assess. Budd offered comprehensive guidance but explicitly noted it was a "clinical practice model," not a standardized instrument — application remained evaluator-dependent. The UK Framework provided domains but was designed for social workers conducting ongoing assessments, not psychologists producing forensic opinions. The capacity-to-change literature addressed prognosis but remained separate from parenting capacity assessment proper. What was missing was integration: a framework that synthesizes these elements into a coherent, operationalized methodology — applying the Structured Professional Judgment approach that has proven effective in violence risk assessment to the parenting assessment context.
That is what PCAF was built to do.
Developing the Parental Capacity Assessment Framework (PCAF) : First Principles from a Decade of Practice
In my decade conducting parental capacity evaluations — for both private custody matters and county DSS permanency planning — and routinely reviewing the work product of other evaluators when retained for secondary opinions, I observed a pattern: the same methodological failures appeared repeatedly, not because individual evaluators were incompetent, but because the field lacked the structured tools that other forensic domains take for granted.
The problems were predictable:
Evaluations that list diagnoses without establishing functional impact on parenting
Reports that assess parenting in a vacuum, disconnected from the specific child's needs
One-sided risk analyses that catalog deficits without systematically identifying protective factors
Static assessments that describe current functioning without addressing capacity for change
Conclusions that bury answers under jargon instead of directly addressing the court's questions
These weren't idiosyncratic failures. They were the natural result of a field without structured methodology.
But my experience revealed something more — three additional realities that any defensible methodology must overcome. These principles, supported by the research literature, fundamentally shaped how we developed PCAF.
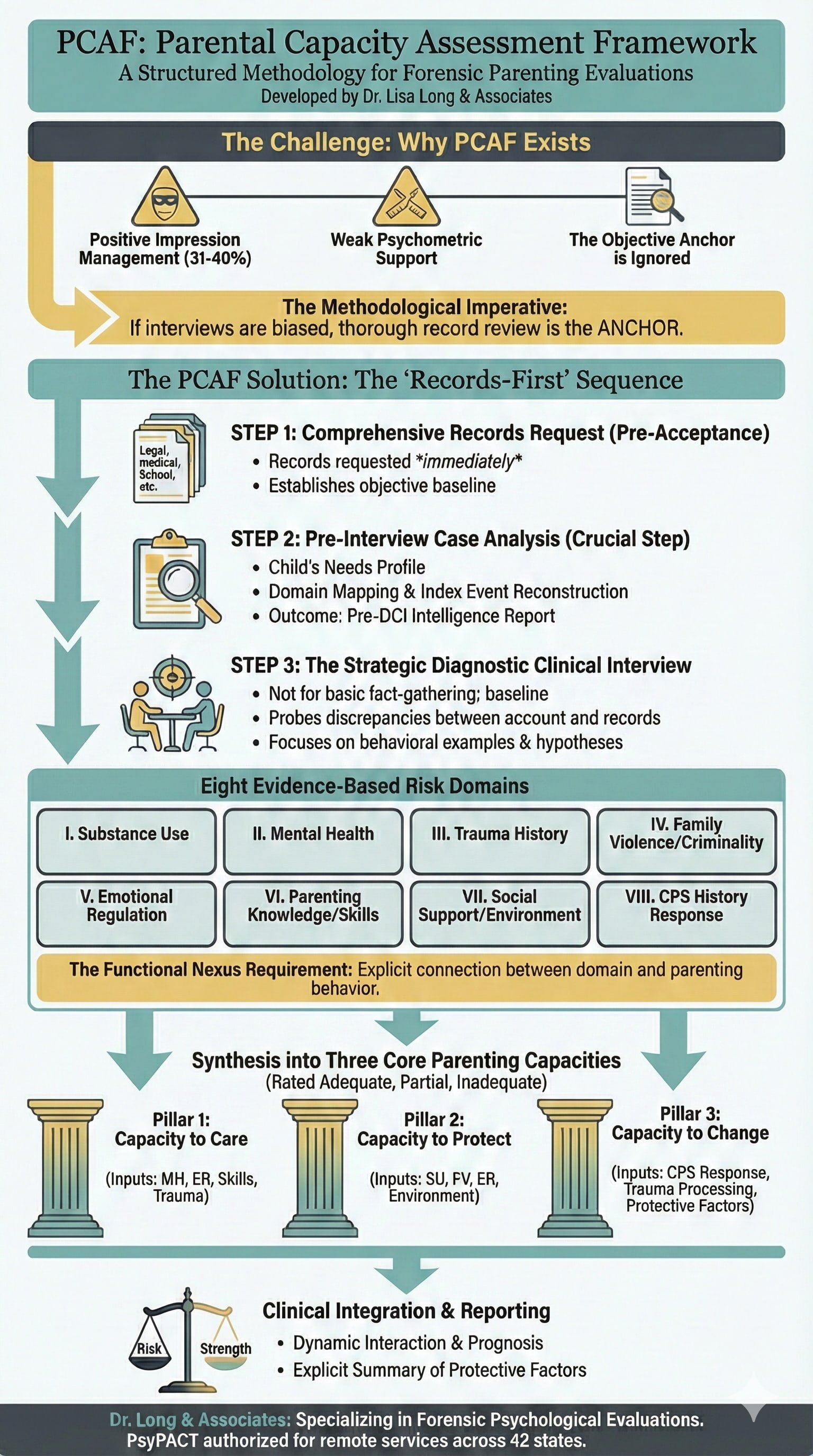
Principle 1: Positive Impression Management Is Pervasive
Parents undergoing custody or parenting-capacity evaluations systematically present themselves in the best possible light. This is not surprising — it is a predictable, even biologically understandable response to a high-stakes assessment that could determine whether you keep your children. But it creates a significant methodological problem.
Taxometric research estimates that 31-40% of parents in custody litigation constitute a distinct "impression management" subgroup who actively manage their presentation (Strong et al., 1999). A meta-analysis of 32 MMPI-2 studies found large effects on validity scales across both custody disputes and child protection cases, confirming that systematic positive self-presentation is "the norm rather than the exception" in these settings (Fariña et al., 2017).
The consequence is predictable: parents in custody evaluations report significantly fewer clinical symptoms than community comparison samples, produce profiles with essentially no clinical-range elevations, and overendorse traits associated with being seen as a good caregiver (Arce et al., 2015). This isn't occasional or limited to certain parents — it's the dominant response pattern in forensic parenting contexts.
This reality carries an important clinical and forensic implication. Positive impression management in parenting evaluations is driven by convergent psychological forces: the biological imperative to protect the parent-child bond, the rational response to a high-stakes assessment with potentially irreversible consequences, and the social desirability pressures inherent in any setting where a person knows they are being evaluated for fitness as a caregiver. These are normal psychological processes, not evidence of pathology.
Yet in my experience consulting on and conducting peer review of other evaluators' work in family law matters, I have encountered evaluations in which elevated impression management indicators on validity scales are treated as evidence that a parent is deceptive, untrustworthy, or lacking in credibility — and in some cases, these elevations are used as standalone factors shaping custody or reunification recommendations. This represents a fundamental misapplication of psychometric data. When the research establishes that systematic positive self-presentation is the normative response pattern in forensic parenting contexts, an evaluator who pathologizes that normed behavior is not identifying a clinical finding — they are penalizing a parent for responding exactly as the population predictably responds. A defensible evaluation must account for impression management methodologically, not weaponize it diagnostically.
Principle 2: Parenting-Specific Instruments Have Weak Psychometric Support
Evaluators have historically relied on instruments like the Child Abuse Potential Inventory (CAPI), Adult-Adolescent Parenting Inventory (AAPI-2), and Parenting Stress Index (PSI-4) to assess parenting-related constructs. The uncomfortable truth is that the evidence base for these instruments is weaker than commonly assumed.
To be clear, instruments such as the CAPI and PSI are not psychometrically worthless. In clinical and research contexts, systematic reviews have found moderate evidence for their validity (Ponticelli et al., 2025; Ríos et al., 2022). The problem is that forensic parenting evaluations represent a significantly more demanding environment for any instrument than clinical or research settings, with pervasive impression management, adversarial context, and life-altering consequences. If the best available evidence supports only moderate validity under favorable conditions, that evidence cannot justify confidence in these instruments under conditions specifically designed to stress their weaknesses.
A systematic review of caregiver-report maltreatment instruments concluded that no instrument, including the AAPI-2, could be recommended as "most suitable" due to lack of high-quality evidence; AAPI-2 remains in the "promising but needs further validation" category (Yoon et al., 2020). A COSMIN-based review rated the CAPI Abuse scale as having only "moderate" overall evidence for validity, with noted methodological limitations (Ponticelli et al., 2025). Available reviews of the PSI suggest generally good internal consistency but limited psychometric data across populations and versions, particularly for the full-length form (Ríos et al., 2022).
More troubling: these instruments are particularly vulnerable to the impression management problem described above. Research in parenting-capacity samples shows that positive self-presentation frequently invalidates MMPI-2, CAPI, and parenting-attitude measures. Experimental research demonstrates that while CAPI validity indices detect 91–95% of fake-good protocols, PSI Defensive Responding identifies fewer than half, leaving evaluators relying on PSI validity scales particularly vulnerable to undetected impression management (Carr et al., 2005; Milner & Crouch, 1997).
The practical implication is uncomfortable but necessary to state directly: given weak psychometric foundations, high vulnerability to impression management, and the empirical reality that no parenting-specific instrument has earned a "most suitable" recommendation from systematic review, evaluators should exercise considerable caution before including these measures in forensic parenting evaluations at all. The conventional defense, that these instruments represent "one data point in a multi-method assessment," is theoretically reasonable but often dishonest in practice. In my experience reviewing other evaluators' work, parenting-specific test scores rarely remain one data point among many. An elevated CAPI Abuse scale or a PSI profile becomes a centerpiece of the clinical narrative, lending a veneer of empirical precision to conclusions that the instrument's own evidence base cannot support. Grisso (1986) identified the core danger in forensic evaluation as the inferential leap from clinical data to forensic opinion without establishing functional connection between the two. Parenting-specific instruments, with their moderate validity evidence and poor impression management detection, are precisely where that leap is most likely to produce indefensible conclusions.
Including an instrument with known psychometric limitations does not strengthen a multi-method assessment. It introduces a data point that is more likely to mislead than inform, and one that judges, attorneys, and caseworkers lack the psychometric training to appropriately discount. A defensible evaluation must justify the inclusion of every measure it administers, not rely on the ritual of 'multi-method assessment' to launder instruments the field's own evidence base cannot fully endorse.
Principle 3: Records Are the Objective Anchor
If interview data is systematically biased by impression management, and testing instruments have weak psychometric support and are vulnerable to the same bias — what data source can an evaluator actually rely on?
The answer is records: documentation created outside the evaluation context, often at times of crisis or stress, when there was no opportunity to manage impressions for an evaluator.
Police reports, CPS investigations, hospital records, school documents, supervised visitation notes — these capture parental functioning in naturalistic contexts. A parent's behavior during a domestic violence incident documented by responding officers, or their engagement during months of supervised visits observed by caseworkers, provides behavioral data that no single interview or test session can match. Records are not presumed to be more accurate than parent accounts — they are one data source among several. Their value lies in providing contemporaneous documentation created outside the evaluation context, which can then be triangulated against interview data, testing results, and collateral information to build a comprehensive clinical picture.
Yet empirical review of actual parenting evaluations reveals a troubling pattern: most reports do not adequately use records or collateral information. Budd and colleagues' analysis of 190 parent evaluations found few prior reports cited, limited behavioral methods employed, and minimal integration of documented history — concluding this was a major weakness in forensic parenting assessment (Budd et al., 2001).
Judges themselves recognize what evaluators often overlook: collateral data about litigants and observations of parent-child interaction are rated among the most useful elements of custody evaluations, more useful than personal references or detailed psychometrics (Axelson & Gentile, 2023).
How PCAF Works: From Domains to Capacities
The three principles above establish a compound methodological problem. Self-report data in forensic parenting evaluations is systematically biased by impression management that the research literature identifies as normative, not aberrant. The parenting-specific instruments available to evaluators carry moderate validity evidence that cannot justify confidence under the adversarial, high-stakes conditions that define forensic practice — and those instruments are themselves vulnerable to the same impression management that contaminates interview data. Records created outside the evaluation context offer the most reliable behavioral evidence, yet empirical review shows most evaluators underutilize them.
These are not problems any single instrument can solve. They are problems that require a structured methodology — one that sequences the evaluation to privilege the most reliable data sources, systematically accounts for impression management rather than ignoring or pathologizing it, and constrains the evaluator's subjectivity at the points where bias is most likely to enter.
Every evaluator conducting parental capacity assessments faces this methodological reality, whether they acknowledge it or not. One option is unstructured clinical judgment: trusting training and experience to guide each evaluation differently depending on the case. Many competent evaluators take this approach, and some do it well. But forensic methodology — and the mentors who shaped my training in it — taught me that unstructured judgment, however experienced, is precisely where bias enters and defensibility erodes. If every other forensic domain demands structured frameworks to constrain subjectivity and ensure systematic analysis, parenting capacity assessment deserves no less.
So I did what the forensic psychology literature prescribes: I studied the empirical research on child maltreatment and child welfare outcomes, identified the domains where consistent associations appear across independent meta-analyses and systematic reviews, and built a structured methodology around them. These domains direct the evaluator not only toward concerns but equally toward strengths, protective factors, and specific intervention targets that improve the likelihood of better outcomes for both parent and child. PCAF's contribution is this structure: eight empirically supported assessment domains, derived from the child maltreatment literature, systematically evaluated and synthesized into three core parenting capacities — through a sequenced workflow designed to mitigate the specific methodological vulnerabilities the field has documented but never adequately addressed.
A critical distinction governs how these domains function within PCAF. The empirical associations that define each domain — between a given risk factor and increased likelihood of harm to children — establish where a competent evaluator is obligated to look. They do not determine what the evaluator will find. Population-level correlations do not predict individual outcomes. The presence of a domain concern does not establish parental incapacity, and the absence of concerns does not guarantee adequate parenting.
The evaluator's task at each domain is twofold. First, determine whether the available evidence — records, collateral information, behavioral observation, clinical interview, and where psychometrically justified, testing — identifies a concern, a strength, or both. Second, and more importantly, determine whether any identified concern has a functional connection to this parent's actual caregiving behavior with this child. Without that demonstrated nexus, a risk indicator is a starting point for investigation, not a basis for conclusions. The same logic applies in the other direction: a protective factor that does not functionally connect to caregiving behavior cannot offset concerns that do. Every domain-level finding, whether it cuts toward risk or toward strength, must earn its place in the analysis through demonstrated relevance to the specific parent-child relationship at issue.
Records-First Methodology
PCAF mandates comprehensive records review as the first substantive step in every evaluation — completed before the diagnostic clinical interview is scheduled. This is not administrative convenience; it is the methodological response to the impression management and measurement problems documented above.
The following sections describe PCAF's operational workflow in sufficient detail for evaluators to understand the sequencing logic and its rationale. Where the tone shifts from argument to protocol, the shift is intentional — a methodology must be specific enough to implement, not merely compelling enough to endorse.
Required Records Request
Upon case acceptance, evaluators request all available documentation, including at minimum:
Legal documents: Petitions, court orders, prior pleadings, custody agreements, GAL reports
Child protective services records: Investigation reports, substantiation findings, case plans, progress notes, prior evaluations
Law enforcement records: Police reports related to index incidents, domestic violence reports, arrest records
Supervised visitation documentation: Visit logs, supervisor observations, incident reports
Treatment records: Mental health treatment notes, substance abuse treatment records, medication management documentation
Medical records: Relevant medical history for parent and child, prenatal records if applicable, emergency room visits related to case concerns
School records: IEPs, 504 plans, teacher observations, disciplinary records, attendance patterns
Collateral documentation: Letters from service providers, employer documentation, housing records
This is not a passive request. Evaluators should work with referring attorneys or caseworkers to identify and obtain records that may not be in the court file — particularly records documenting functioning during crisis periods or at times of stress.
Pre-Interview Case Analysis
Before scheduling the diagnostic clinical interview, the evaluator completes structured analysis of all available records:
Child's Needs Profile: Documented developmental, medical, educational, and psychological needs are extracted from records — establishing the child-specific benchmark against which parenting capacity will be assessed
Preliminary Domain Mapping: Evidence relevant to each of the eight PCAF domains is identified and organized — what do records reveal about substance use history, mental health treatment, trauma indicators, violence history, prior CPS involvement?
Risk and Protective Factor Inventory: Documented risk indicators and protective factors are catalogued by domain, with source citations
Index Event Reconstruction: The documented timeline and facts of the index incident (if applicable) are established from contemporaneous records — police reports, CPS investigation notes, medical records — before the parent provides their account
Strategic Question Development: Based on gaps in the record and areas requiring clarification, specific questions are developed for the diagnostic clinical interview — questions designed to test hypotheses, probe discrepancies, and elicit behavioral examples
This pre-interview analysis produces a Pre-DCI Intelligence Report — a structured briefing document that ensures the evaluator enters the clinical interview with comprehensive case knowledge rather than relying on the parent's account to establish basic facts.
Why This Sequence Matters
The traditional approach — conducting intake interviews first, then reviewing records — inverts the proper methodology. If the evaluator's initial understanding of the case comes from the parent's self-report, that impression-managed account becomes the cognitive anchor against which records are later interpreted. Confirmatory bias operates in the parent's favor.
The records-first approach reverses this dynamic. The evaluator establishes objective baseline facts from contemporaneous documentation. The parent's account is then assessed against this baseline — with discrepancies between documented record and parent report becoming key clinical data rather than being smoothed over or overlooked.
Child-Centered Foundation
With records reviewed and analyzed, the evaluation proceeds to formalize the child-centered foundation. Before analyzing any parental risk domains, PCAF requires comprehensive documentation of the specific child's needs:
Developmental stage and milestones
Medical and health requirements
Educational needs (IEP, special education, academic challenges)
Psychological and emotional needs (trauma history, mental health, attachment patterns)
Special needs and vulnerabilities
This child-first sequencing fundamentally reframes the evaluation. The question is not "Is this a good parent?" — an abstraction that invites evaluator bias. The question is: "Can this parent meet this specific child's needs?"
A parent who demonstrates adequate capacity for a typically developing eight-year-old may lack the specialized knowledge, emotional regulation, and medical management skills required to safely parent a four-year-old with autism spectrum disorder and a seizure disorder. Without establishing the child's needs profile first, the evaluation lacks the context necessary for meaningful assessment.
Eight Evidence-Based Risk Domains
Following child-needs assessment, PCAF organizes parental evaluation around eight domains. These are not arbitrary categories. Each represents an area identified across multiple independent systematic reviews, meta-analyses, and longitudinal cohort studies as warranting structured professional assessment in the context of parenting capacity evaluation. Each domain is evaluated under the interpretive framework described above — investigating for both concerns and strengths, with every finding required to demonstrate functional connection to this parent's caregiving behavior before it carries analytic weight.
Domain I: Parental Substance Use
Assessment of alcohol and drug use patterns, functional impact on parenting, treatment engagement, and relapse prevention. The critical analytic task is establishing nexus: the specific connection between substance use and parenting deficits, rather than equating any substance use with incapacity. A positive toxicology screen is a data point, not a conclusion.
Protective factors to assess: Sustained sobriety with documented clean date; active engagement in treatment or recovery community; articulated relapse prevention plan with child safety measures; insight into how substance use affected parenting; pro-social sober support network.
Domain II: Mental Health and Psychological Functioning
Evaluation of psychiatric disorders, personality functioning, and cognitive abilities as they impact parenting. The focus is functional impairment: how do symptoms manifest in specific parenting behaviors? Diagnosis is a risk marker, not a risk factor. A well-managed bipolar disorder may pose less concern than untreated subclinical depression that causes chronic emotional unavailability.
Protective factors to assess: Consistent medication compliance with symptom stability; active therapeutic engagement; demonstrated insight into illness and its impact on the child; documented periods of stability; ability to identify warning signs and implement coping strategies.
Domain III: Parent's History of Trauma and Maltreatment
Assessment of the parent's own childhood experiences and their current impact on parenting. The key analytic distinction is between resolved and unresolved trauma. Resolved trauma is characterized by a parent who has processed their history, reflects on it with emotional distance, and consciously parents differently. Unresolved trauma carries the risk of intergenerational transmission, where harmful patterns are unconsciously repeated.
Protective factors to assess: Engagement in trauma-focused therapy; ability to reflect on childhood experiences without emotional flooding; explicit commitment to parenting differently with behavioral evidence of follow-through; demonstrated breaks in intergenerational patterns; strong reflective functioning capacity.
Domain IV: History of Family Violence and Criminal Offending
Examination of intimate partner violence and criminal involvement. Analysis focuses on pattern, nature, severity, and recency, with particular attention to the parent's current attitude toward their history. The forensically relevant question is accountability versus minimization.
Protective factors to assess: Accountability without victim-blaming; completion of batterer intervention or relevant treatment; sustained period without incidents; severed ties with antisocial associates; removal from the relationship or environment that contributed to violence; empathy for those affected.
Domain V: Emotional Regulation and Coping
Assessment of the parent's capacity to manage stress, frustration, and intense emotion, particularly in response to child-specific triggers. The question is not whether a parent experiences stress but how they manage it within the parenting role. The critical analytic distinction here parallels the impression management problem that runs through the entire methodology: what a parent demonstrates in a structured evaluation setting — calm, composed, articulate about coping strategies — may bear little resemblance to how they function at 2:00 a.m. with a screaming toddler, an overdue electric bill, and no support. The evaluator's task is to look past the regulated interview presentation and triangulate against documented behavioral data: police reports describing escalation under stress, supervised visit notes capturing real-time reactions, or CPS records documenting what happened when coping actually failed. Self-reported coping repertoires are hypotheses to be tested against the record, not findings to be documented at face value.
Protective factors to assess: Demonstrated ability to de-escalate when frustrated; use of adaptive coping strategies (support-seeking, breaks, relaxation); capacity to repair after ruptures with the child; self-awareness of triggers; proactive stress management rather than reactive crisis response.
Domain VI: Parenting Knowledge, Beliefs, and Skills
Evaluation of developmental understanding, discipline philosophy, and demonstrated abilities. The critical analytic distinction is the knowledge-to-practice gap — and the frequency with which evaluators fail to assess it. A certificate of completion from a parenting education program demonstrates exposure to material, not acquisition of skill. In my review experience, completed parenting classes are routinely cited in evaluations as evidence of improved parenting capacity, when they are actually evidence only that the parent attended. The forensically relevant question is skill transfer under ecological conditions: can this parent implement what they learned when the child is dysregulated, the environment is chaotic, and there is no instructor providing prompts? Observed parent-child interaction, particularly during unstructured or mildly stressful tasks, provides data that no self-report or course completion certificate can match.
Protective factors to assess: Age-appropriate developmental expectations; consistent use of positive discipline strategies; demonstrated warmth, sensitivity, and attunement in observations; successful completion of parenting education with observable skill transfer; willingness to accept guidance and implement feedback.
Domain VII: Social Support and Environmental Context
Assessment of the parent's support network and environmental stability. The key analytic task is distinguishing between supports that function protectively and supports that enable concerning behavior — a distinction that requires the evaluator to look past the surface presentation of a support network. A grandmother who pledges to supervise visits but has historically minimized the parent's substance use is not a protective factor; she is an additional risk variable. Family members who testify to the parent's improvement while the documented record shows ongoing concerns are not evidence of a support network — they are evidence of a system that reinforces the parent's impression-managed narrative. The evaluator must assess not merely who is present in a parent's life, but what those individuals have actually done when the parent's functioning deteriorated, and whether their involvement correlates with improved or worsened outcomes for the child.
Protective factors to assess: Reliable pro-social support network with documented history of constructive involvement; stable housing and employment; willingness to accept help; engagement with community resources; sober and supportive partner or family involvement; sufficient resources to meet the child's basic needs.
Domain VIII: History of Child Protection Involvement
Review of all prior CPS reports, substantiations, and service engagement. The forensically relevant information is the parent's response to past intervention, and the critical analytic distinction is between compliance and internalized change. A parent who completes every element of a service plan — attends every session, submits every drug screen, checks every box — has demonstrated the ability to follow instructions under external monitoring. That is not the same as demonstrating change. The evaluator's task is to differentiate mechanical compliance from meaningful engagement by examining what happened when monitoring decreased. Did the behavioral gains persist after the case closed? Did the parent seek continued services voluntarily or only under court order? A pattern in which functioning improves during active CPS involvement and deteriorates after case closure is among the most diagnostically significant findings in this domain — it suggests that the parent's behavioral capacity is contingent on external structure rather than reflective of internalized skill.
Protective factors to assess: Successful completion of prior case plans with sustained behavioral change beyond the monitoring period; demonstrated insight into what led to agency involvement; proactive engagement with services rather than mere compliance; maintained stability since last involvement; voluntary continuation of beneficial services after case closure.
The Strategic Diagnostic Clinical Interview
With records analyzed and domains mapped, the diagnostic clinical interview serves a different function than traditional intake interviews. The evaluator is not gathering basic history from scratch — that baseline is already established from documentation. Instead, the interview is strategically designed to:
Gather Standard Historical Information: Developmental history, family of origin, relationship history, educational and vocational background, medical and psychiatric history — the standard elements of a comprehensive clinical interview remain essential. But the evaluator already knows what the records show in these areas, allowing for targeted follow-up on gaps and inconsistencies.
Probe Index Event Accounts: The parent's narrative of the index incident is elicited and compared against the documented timeline established from contemporaneous records. Discrepancies in timing, sequence, severity, or causation are noted and explored — not accusatorially, but as clinical data about the parent's insight, accountability, and cognitive processing of events.
Test Domain-Specific Hypotheses: Strategic questions developed during pre-interview analysis target specific risk and protective factors. Rather than generic inquiries ("Tell me about your substance use"), questions are tailored to documented concerns ("Records show three positive toxicology screens between March and July. Walk me through what was happening during that period and how you understand those results").
Assess Insight and Accountability: How does the parent explain documented concerns? Do they acknowledge problems and demonstrate understanding of impact on the child? Do they externalize blame, minimize severity, or demonstrate genuine reflection? These patterns — assessed against documented facts — inform the capacity-to-change analysis.
Elicit Behavioral Examples: For each domain, the interview seeks specific behavioral examples of both risk indicators and protective factors. Not "Are you a good parent?" but "Describe the last time your child had a meltdown in public. Walk me through exactly what happened and how you handled it."
The result is a clinical interview that is simultaneously thorough and efficient — covering comprehensive history while focusing clinical attention on the issues that actually matter for this specific case and this specific child.
Functional Nexus Requirement
For each domain, PCAF mandates that evaluators:
Document both risk indicators AND protective factors (balanced analysis)
Establish explicit functional nexus between characteristics and specific parenting behaviors
Gather converging evidence from multiple methods and sources
Avoid the logical fallacy of equating diagnosis or characteristics with parental incapacity
This functional approach prevents the most common evaluation failure: listing risk factors without explaining their impact. A positive drug screen is a data point. How that substance use specifically compromised supervision, emotional availability, or child safety is the forensically relevant information.
Synthesis into Three Core Capacities
Following comprehensive domain analysis, findings are synthesized into three functional parenting capacities. Each capacity receives a structured classification — Adequate, Partial, or Inadequate — with detailed rationale explaining how the evidence supports the classification.
Capacity to Care
The parent's ability to meet the child's emotional, developmental, and physical needs through attunement, nurturing, and responsive parenting.
Primary Informing Domains:
Domain II (Mental Health) — Psychiatric symptoms affecting emotional availability, attunement, consistency
Domain V (Emotional Regulation) — Ability to remain regulated and responsive under parenting stress
Domain VI (Parenting Knowledge/Skills) — Developmental expectations, warmth, discipline philosophy, knowledge-to-practice transfer
Domain III (Trauma History) — Resolved vs. unresolved trauma affecting attachment capacity and emotional presence
Rating Anchors:
Adequate: Demonstrates consistent warmth, attunement, age-appropriate expectations; mental health stable or well-managed; emotional regulation sufficient to maintain responsiveness under typical parenting stress
Partial: Capacity present but inconsistent; symptoms or dysregulation intermittently compromise availability; parenting knowledge present but implementation gaps under stress
Inadequate: Chronic emotional unavailability; unmanaged psychiatric symptoms directly impairing caregiving; persistent inability to attune to child's developmental or emotional needs
Capacity to Protect
The parent's ability to keep the child safe from harm — including from their own behavior, environmental risks, and third parties.
Primary Informing Domains:
Domain I (Substance Use) — Impaired judgment, neglect risk, exposure to dangerous situations or people
Domain IV (Family Violence/Criminal History) — Direct harm risk, pattern of exposing child to violence, accountability vs. minimization
Domain V (Emotional Regulation) — Risk of discipline escalation, emotional abuse, loss of control
Domain VII (Social Support/Environment) — Quality of people with access to child, environmental stability, ability to screen unsafe individuals
Rating Anchors:
Adequate: Demonstrates protective vigilance; substance use absent or poses no functional risk; no recent violence/criminal involvement with accountability for past; support network is pro-social; identifies and excludes unsafe individuals
Partial: Protective capacity compromised in specific domains (e.g., history of poor partner selection, early recovery with limited track record); requires monitoring or structured supports to maintain safety
Inadequate: Active substance use impairing supervision/judgment; ongoing violence exposure or minimization of past harm; environmental chaos or access by known unsafe individuals; cannot reliably prioritize child safety over adult relationships
Capacity to Change
The parent's amenability to intervention, insight, and demonstrated ability to make and sustain meaningful behavioral change.
Primary Informing Domains:
Domain VIII (CPS History) — Response to past intervention; compliance vs. meaningful engagement; sustained change vs. repeated concerns
Domain III (Trauma History) — Evidence of processing, insight, breaking intergenerational patterns
Protective factors across all domains — Treatment engagement, accountability, insight, relapse prevention planning, self-awareness
Secondary Contributors:
Domain II (Mental Health) — Treatment compliance, insight into symptoms, self-monitoring capacity
Domain I (Substance Use) — Recovery trajectory, relapse prevention sophistication, length of sustained sobriety
Rating Anchors:
Adequate: Demonstrated sustained behavioral change over meaningful time period; insight into past deficits; proactive (not merely compliant) engagement with services; articulates specific strategies to maintain gains; breaks from prior patterns evident
Partial: Early-stage change with limited track record; insight present but inconsistent; compliance without internalization; change in some domains but not others
Inadequate: Pattern of non-engagement or superficial compliance; repeated CPS involvement without sustained improvement; minimization, externalization, or lack of insight; no evidence change will persist without external monitoring
Clinical Integration
The three capacities are not independent — they interact dynamically. A parent with adequate capacity to care but partial capacity to protect (e.g., poor partner selection history) may still present unacceptable risk. A parent with partial capacity to care but adequate capacity to change may be a strong reunification candidate with appropriate services. Inadequate capacity to change often drives prognosis regardless of current functioning in other domains.
The evaluator's ultimate opinion synthesizes across all three capacities, weighted by the specific risk factors present in the case and the child's particular vulnerabilities. Critically, that synthesis must account for what resources exist to mitigate identified risk — not only what places a child in danger, but what might reduce that danger. A parent with significant risk factors who also demonstrates strong insight, active treatment engagement, and a robust pro-social support network presents a fundamentally different clinical picture than a parent with identical risks and no protective factors. Courts need both sides of that analysis to make informed decisions, which is why PCAF's integration of protective factors and strengths throughout every domain and every capacity rating — rather than as a separate afterthought — is structurally essential to the framework's claim of balanced analysis.
Selecting an Evaluator: What to Look For
When requesting a parental capacity evaluation — whether for private litigation or child welfare proceedings — consider asking potential evaluators:
What framework or methodology guides your evaluations? Evaluators should be able to articulate a systematic approach. Vague references to "clinical judgment" without structured methodology should raise concerns.
How do you establish the connection between diagnoses or characteristics and actual parenting behavior? Look for evaluators who emphasize functional analysis — what parents do, not just what diagnoses they carry.
Do you systematically assess protective factors, or primarily document deficits? Quality evaluations require balanced analysis.
How do you assess capacity for change? Static snapshots of current functioning are insufficient for permanency planning or determining what services might help.
Will your report directly answer the referral questions? The purpose of an evaluation is to inform specific decisions. Reports should be organized to address those decisions directly.
What is your records review process? Evaluators who conduct interviews before thoroughly reviewing records are inverting the proper methodology.
A Note on Framework Status
PCAF is an evidence-informed Structured Professional Judgment framework — not a psychometrically validated instrument. No such instrument exists in parental capacity assessment; this methodological gap has been documented in the literature for over two decades (Budd, 2001, 2005). PCAF addresses that gap by applying SPJ principles — systematic domain coverage, structured risk and protective factor analysis, and explicit synthesis procedures — to parenting assessment.
The framework is built on three first principles derived from the empirical literature: (1) positive impression management is pervasive in forensic parenting contexts, (2) parenting-specific instruments have weak psychometric support, and (3) contemporaneous records provide the most reliable behavioral data. These principles are not merely background — they are the design rationale that shaped PCAF's methodology, including its records-first workflow, cautious integration of testing data, and emphasis on multi-source triangulation.
The framework's eight risk domains are derived from empirical literature, including meta-analyses and systematic reviews of child maltreatment risk factors. The three-capacity synthesis and rating anchors were developed through clinical practice — over a decade of conducting evaluations and reviewing the work product of other evaluators across both private custody and child welfare contexts.
PCAF is discretionary: it structures and guides professional judgment but does not replace it. Evaluators apply clinical expertise to weigh evidence, interpret findings, and formulate opinions. The framework's value lies in ensuring systematic, transparent, and empirically-grounded assessment — a meaningful improvement over the unstructured approaches that remain common in the field.
About Our Practice
At Dr. Long & Associates, we specialize in forensic psychological evaluations for family law and child welfare contexts. I developed the Parental Capacity Assessment Framework (PCAF) through over a decade of forensic practice — conducting evaluations for both private custody matters and county DSS permanency planning — synthesizing established research traditions with hard-won clinical expertise to create the structured methodology the field has lacked.
I am PsyPACT authorized (#8593), enabling remote evaluation services across 42 participating states. We prioritize referrals from government agencies and typically complete evaluations within 3-4 weeks of the evaluation appointment.
Need a parental capacity evaluation or consultation?
Explore Our Services: Court-Ordered Psychological Evaluation Services
Request a Fast Response: 24-Hour Referral Request Portal
Professional Disclaimer — Parental Capacity Evaluations
This article is provided for educational purposes only and does not constitute legal advice, psychological services, or a professional consultation. The information presented reflects general principles in forensic psychology and should not be applied to any specific case without consultation with a qualified forensic psychologist and legal counsel.
The Parental Capacity Assessment Framework (PCAF) described herein is an evidence-informed clinical framework, not a psychometrically validated instrument. Individual evaluation outcomes depend on case-specific facts and circumstances.
Dr. Lisa Long is a licensed psychologist authorized to practice via PSYPACT (APIT #8593) in 42 U.S. states and jurisdictions. Jurisdictional limitations may apply. Reading this article does not establish a psychologist-client relationship.
If you enjoyed this comprehensive guide on evaluating parental capacity, you may also appreciate the following related resources.
👉Understanding When You Need a Psychological, Parental Capacity, or Custody Evaluation
References
First Principles Research
Arce, R., Fariña, F., Seijo, D., & Novo, M. (2015). Assessing impression management with the MMPI-2 in child custody litigation. Assessment, 22, 769-777. https://doi.org/10.1177/1073191114558111
Axelson, T., & Gentile, J. (2023). Are child custody evaluations beneficial to family law judges? A study from the judicial perspective. Family Court Review, 61(4), 715-729. https://doi.org/10.1111/fcre.12772
Budd, K. S., Poindexter, L. M., Felix, E. D., & Naik-Polan, A. T. (2001). Clinical assessment of parents in child protection cases: An empirical analysis. Law and Human Behavior, 25, 93-108. https://doi.org/10.1023/a:1005696026973
Carr, G. D., Moretti, M. M., & Cue, B. J. H. (2005). Evaluating parenting capacity: Validity problems with the MMPI-2, PAI, CAPI, and ratings of child adjustment. Professional Psychology: Research and Practice, 36, 188-196. https://doi.org/10.1037/0735-7028.36.2.188
Fariña, F., Redondo, L., Seijo, D., Novo, M., & Arce, R. (2017). A meta-analytic review of the MMPI validity scales and indexes to detect defensiveness in custody evaluations. International Journal of Clinical and Health Psychology, 17, 128-138. https://doi.org/10.1016/j.ijchp.2017.02.002
Ponticelli, S., Martin, P., & Sleed, M. (2025). A systematic review and critical appraisal of the psychometric properties of the Child Abuse Potential Inventory (CAPI). Child Maltreatment. https://doi.org/10.1177/10775595251329298
Ríos, M., Zekri, S., Alonso-Esteban, Y., & Navarro-Pardo, E. (2022). Parental stress assessment with the Parenting Stress Index (PSI): A systematic review of its psychometric properties. Children, 9(11), 1649. https://doi.org/10.3390/children9111649
Strong, D. R., Greene, R. L., Hoppe, C., Johnston, T., & Olesen, N. (1999). Taxometric analysis of impression management and self-deception on the MMPI-2 in child custody litigants. Journal of Personality Assessment, 73(1), 1-18. https://doi.org/10.1207/s15327752jpa730101
Yoon, S., Speyer, R., Cordier, R., Aunio, P., & Hakkarainen, A. (2020). A systematic review evaluating psychometric properties of parent or caregiver report instruments on child maltreatment: Part 2. Trauma, Violence, & Abuse, 22(5), 1296-1315. https://doi.org/10.1177/1524838020915591
Foundational Literature
Azar, S. T., Lauretti, A. F., & Loding, B. V. (1998). The evaluation of parental fitness in termination of parental rights cases: A functional-contextual perspective. Clinical Child and Family Psychology Review, 1, 77-100.
Budd, K. S. (2001). Assessing parenting competence in child protection cases: A clinical practice model. Clinical Child and Family Psychology Review, 4(1), 1-18.
Budd, K. S. (2005). Assessing parenting capacity in a child welfare context. Children and Youth Services Review, 27, 429-444.
Budd, K. S., & Holdsworth, M. J. (1996). Issues in clinical assessment of minimal parenting competence. Journal of Clinical Child Psychology, 25(1), 2-14.
Department of Health. (2000). Framework for the Assessment of Children in Need and their Families. London: The Stationery Office.
Grisso, T. (1986). Evaluating competencies: Forensic assessments and instruments. New York: Plenum Press.
Harnett, P. H. (2007). A procedure for assessing parents' capacity for change in child protection cases. Children and Youth Services Review, 29, 1179-1188.
Platt, D., & Riches, K. (2016). Assessing parental capacity to change: The missing jigsaw piece in the assessment of a child's welfare? Children and Youth Services Review, 61, 141-148.
PCAF Risk Domain Evidence Base
PCAF Risk Domain Evidence Base
The following citations represent the primary empirical support for each of PCAF's eight assessment domains. Each domain is supported by systematic reviews and meta-analyses demonstrating sufficient empirical consensus to warrant structured professional assessment within a parental capacity evaluation framework.
Domain I — Parental Substance Use
Kuppens, S., Moore, S. C., Gross, V., & Lowthian, E. (2020). The enduring effects of parental alcohol, tobacco, and drug use on child well-being: A multilevel meta-analysis. Development and Psychopathology, 32(2), 765–778. https://doi.org/10.1017/S0954579419000749
Luo, Z., Chen, Y., & Epstein, R. A. (2025). Risk factors for child abuse and neglect: Systematic review and meta-analysis. Public Health. https://doi.org/10.1016/S0033-3506(25)00049-6
Norman, R. E., Byambaa, M., De, R., & Butchart, A. (2012). The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis. PLoS Medicine, 9(11), e1001349. https://doi.org/10.1371/journal.pmed.1001349
Domain II — Mental Health and Psychological Functioning
Ayers, S., Bond, R., Webb, R., Miller, P., & Bateson, K. (2019). Perinatal mental health and risk of child maltreatment: A systematic review and meta-analysis. Child Abuse & Neglect, 98, 104172. https://doi.org/10.1016/j.chiabu.2019.104172
Nielsen, T. T., Bali, P., Grove, J., & Mohr-Jensen, C. (2025). Genetic architecture and risk of childhood maltreatment across 5 psychiatric diagnoses. JAMA Psychiatry. https://doi.org/10.1001/jamapsychiatry.2025.0435
Senberg, A., Schmucker, M., Oster, A., & Zumbach, J. (2023). Parental personality disorder and child maltreatment: A systematic review and meta-analysis. Child Abuse & Neglect, 143, 106278. https://doi.org/10.1016/j.chiabu.2023.106278
Domain III — Parent's History of Trauma and Maltreatment
Assink, M., Spruit, A., Schuts, M., & Lindauer, R. (2018). The intergenerational transmission of child maltreatment: A three-level meta-analysis. Child Abuse & Neglect, 84, 131–145. https://doi.org/10.1016/j.chiabu.2018.07.037
Madigan, S., Cyr, C., Eirich, R., & Fearon, R. M. P. (2019). Testing the cycle of maltreatment hypothesis: Meta-analytic evidence of the intergenerational transmission of child maltreatment. Development and Psychopathology, 31(1), 23–51. https://doi.org/10.1017/S0954579418001700
Savage, L. É., Tarabulsy, G. M., & Pearson, J. (2019). Maternal history of childhood maltreatment and later parenting behavior: A meta-analysis. Development and Psychopathology, 31(1), 9–21. https://doi.org/10.1017/S0954579418001542
Domain IV — History of Family Violence and Criminal Offending
Chiesa, A. E., Kallechey, L., Harlaar, N., & Ford, C. R. (2018). Intimate partner violence victimization and parenting: A systematic review. Child Abuse & Neglect, 80, 285–300. https://doi.org/10.1016/j.chiabu.2018.03.028
Chan, K. L., Chen, Q., & Chen, M. (2021). Prevalence and correlates of the co-occurrence of family violence: A meta-analysis on family polyvictimization. Trauma, Violence, & Abuse, 22(2), 289–305. https://doi.org/10.1177/1524838019841601
Mulder, T. M., Kuiper, K. C., van der Put, C. E., & Stams, G. J. J. M. (2018). Risk factors for child neglect: A meta-analytic review. Child Abuse & Neglect, 77, 198–210. https://doi.org/10.1016/j.chiabu.2018.01.006
Domain V — Emotional Regulation and Coping
Lavi, I., Ozer, E. J., Katz, L. F., & Gross, J. J. (2021). The role of parental emotion reactivity and regulation in child maltreatment and maltreatment risk: A meta-analytic review. Clinical Psychology Review, 90, 102099. https://doi.org/10.1016/j.cpr.2021.102099
Zimmer-Gembeck, M. J., & Rudolph, J. (2022). Parent emotional regulation: A meta-analytic review of its association with parenting and child adjustment. International Journal of Behavioral Development, 46(1), 63–82. https://doi.org/10.1177/01650254211051086
Lavi, I., Manor-Binyamini, I., Seibert, E., & Katz, L. F. (2019). Broken bonds: A meta-analysis of emotion reactivity and regulation in emotionally maltreating parents. Child Abuse & Neglect, 88, 376–388. https://doi.org/10.1016/j.chiabu.2018.11.016
Domain VI — Parenting Knowledge, Beliefs, and Skills
Gubbels, J., van der Put, C. E., & Assink, M. (2019). The effectiveness of parent training programs for child maltreatment and their components: A meta-analysis. International Journal of Environmental Research and Public Health, 16(13), 2404. https://doi.org/10.3390/ijerph16132404
Van der Put, C. E., Assink, M., & Gubbels, J. (2018). Identifying effective components of child maltreatment interventions: A meta-analysis. Clinical Child and Family Psychology Review, 21(2), 171–202. https://doi.org/10.1007/s10567-017-0250-5
Younas, F., & Gutman, L. M. (2023). Parental risk and protective factors in child maltreatment: A systematic review of the evidence. Trauma, Violence, & Abuse, 24(5), 3526–3543. https://doi.org/10.1177/15248380221134634
Domain VII — Social Support and Environmental Context
Assink, M., Van der Put, C. E., & Meeuwsen, M. W. C. M. (2019). Risk factors for child sexual abuse victimization: A meta-analytic review. Psychological Bulletin, 145(5), 459–489. https://doi.org/10.1037/bul0000188
White, O. G., & Hindley, N. (2015). Risk factors for child maltreatment recurrence: An updated systematic review. Medicine, Science and the Law, 55(4), 259–277. https://doi.org/10.1177/0025802414543855
Younas, F., & Gutman, L. M. (2023). Parental risk and protective factors in child maltreatment: A systematic review of the evidence. Trauma, Violence, & Abuse, 24(5), 3526–3543. https://doi.org/10.1177/15248380221134634
Domain VIII — History of Child Protection Involvement
Hindley, N., & Ramchandani, P. G. (2006). Risk factors for recurrence of maltreatment: A systematic review. Archives of Disease in Childhood, 91(9), 744–752. https://doi.org/10.1136/adc.2005.085639
Kim, H., & Drake, B. (2019). Cumulative prevalence of onset and recurrence of child maltreatment reports. Journal of the American Academy of Child & Adolescent Psychiatry, 58(12), 1175–1183. https://doi.org/10.1016/j.jaac.2019.02.015
White, O. G., & Hindley, N. (2015). Risk factors for child maltreatment recurrence: An updated systematic review. Medicine, Science and the Law, 55(4), 259–277. https://doi.org/10.1177/0025802414543855
The Parental Capacity Assessment Framework (PCAF) — a structured, records-first methodology for forensic parenting evaluations addressing impression management bias and weak psychometric support in traditional approaches.
Lisa Long, PsyD | Dr. Long & Associates