
How Independent Psychological Evaluations Strengthen Social Security Disability Claims for Mental Health Conditions
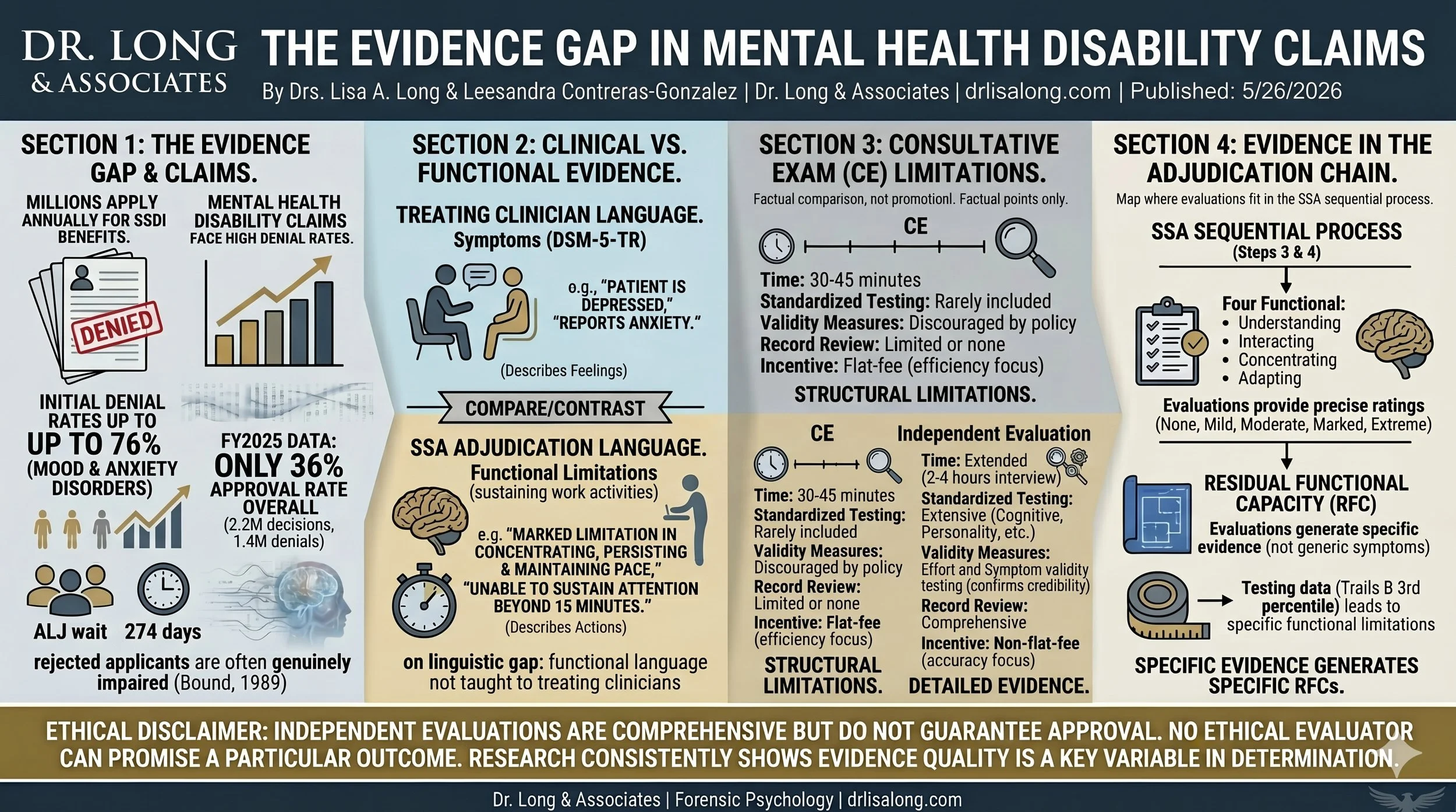
An informational infographic by forensic psychologists Dr. Lisa A. Long and Dr. Leesandra Contreras-Gonzalez detailing the evidence gap in mental health SSDI claims. The graphic illustrates high initial denial rates, contrasts treating clinicians' symptom-based language with the SSA's functional limitation language, and outlines the structural limitations of brief consultative exams (CEs). It concludes by showing how comprehensive independent psychological evaluations provide objective testing data for precise Residual Functional Capacity (RFC) assessments. Produced by Dr. Long & Associates.
Authors: Lisa A. Long, Psy.D., Leesandra Contreras-Gonzalez, Psy.D.
Dr. Long & Associates | drlisalong.com
Published: 5/26/2026
Attorneys and claimants can request an evaluation here.
1. Introduction: The Evidence Gap in Mental Health Disability Claims
Every year, millions of Americans apply for Social Security Disability Insurance (SSDI) benefits after a disabling medical condition prevents them from working. For applicants with mental health conditions — major depression, anxiety disorders, PTSD, bipolar disorder, cognitive impairment — the process is especially difficult. Research consistently shows that mental health claims are denied at significantly higher rates than other categories of disability, with studies finding denial rates as high as 76% for mood and anxiety disorders at the initial application stage (Autor & Duggan, 2006; Deshpande & Li, 2019).
In fiscal year 2025, the Social Security Administration (SSA) approved only 36% of all initial disability applications — a nearly three-percentage-point drop from the prior year's 38.7% approval rate. Out of 2,246,542 initial decisions, nearly 1.44 million applicants were denied. For those who appeal to an Administrative Law Judge (ALJ), the national average wait is approximately 274 days. During that wait, many claimants — already unable to work — exhaust savings, lose housing, and deteriorate further (Christensen et al., 2019; Deshpande & Li, 2019).
These denials are not primarily the result of applicants who aren't really disabled. Bound's (1989) landmark study found that fewer than 50% of rejected disability applicants returned to work, and those who did earned less than half the median income for their age group. The rejected population is, by and large, genuinely impaired. The problem is not the severity of the condition — it is the quality and specificity of the evidence in the file.
This is the gap that independent psychological evaluations are designed to fill. Conducted by licensed psychologists with training in forensic assessment methodology, these evaluations produce comprehensive documentation that addresses the specific functional questions SSA needs answered — documentation that SSA's own evaluation process often fails to generate. This article explains why the gap exists, what independent evaluations provide, and how they fit into the disability adjudication process.
This article is not a guarantee of any particular outcome. No ethical evaluator can promise that an evaluation will result in approval of benefits. What the research consistently shows, however, is that the quality and specificity of psychological evidence is one of the most significant variables in disability determination — and that SSA's own mechanisms for generating that evidence are structurally limited.
2. Why Mental Health Disability Claims Are Denied at Higher Rates
Mental health conditions present unique challenges for disability adjudication that physical conditions do not. Understanding these challenges is essential for claimants, attorneys, and clinicians who want to build the strongest possible evidentiary record.
2.1 The Invisibility Problem
A fractured spine shows up on an MRI. A torn rotator cuff appears on imaging. Heart disease produces abnormal EKG findings. Mental health conditions produce none of these objective markers. There is no blood test for depression, no scan that shows anxiety, no biopsy that confirms PTSD. The diagnosis rests on clinical judgment — the evaluator's synthesis of self-reported symptoms, behavioral observations, collateral data, and standardized testing.
This does not make mental health diagnoses less valid. The DSM-5-TR diagnostic criteria for major depressive disorder, generalized anxiety disorder, and post-traumatic stress disorder are supported by decades of research, field testing, and clinical validation. But it does mean that mental health evidence requires a different kind of documentation than physical health evidence — documentation that many treating clinicians are not trained or equipped to provide in the format SSA requires.
2.2 The Fluctuation Problem
Mental health conditions fluctuate. A person with major depressive disorder may have weeks where they can manage basic tasks and days where they cannot get out of bed. A person with PTSD may function adequately in low-stress environments but decompensate under the sustained demands of competitive employment. A person with bipolar disorder may present as organized and articulate during a hypomanic phase and be unable to concentrate or make decisions during a depressive episode.
SSA's evaluation process — particularly the consultative examination, discussed in Section 4 — captures a single point in time. A 40-minute examination on a relatively functional day can produce a report suggesting the claimant's limitations are only "moderate" when, over the course of weeks and months, functioning is severely impaired. The snapshot does not capture the pattern.
2.3 The Vocabulary Problem
Perhaps the most consequential gap is linguistic. Treating clinicians — therapists, psychiatrists, primary care physicians — document mental health conditions using clinical language: "patient reports persistent low mood," "affect was constricted," "sleep is disrupted." This language describes symptoms. SSA does not make disability determinations based on symptoms alone. SSA evaluates functional limitations — the specific ways a mental health condition prevents someone from performing work-related activities on a sustained basis.
The four functional areas SSA evaluates (discussed in detail in Section 3) require evidence stated in terms of what the claimant can and cannot do, not what they feel. A treatment note that says "patient is depressed" tells the adjudicator very little. A report that says "the claimant's depressive disorder produces marked limitation in the ability to concentrate, persist, and maintain pace, as evidenced by an inability to sustain focused attention for more than 15 minutes, consistent errors on tasks requiring sustained concentration, and a documented pattern of incomplete or abandoned daily activities" gives the adjudicator the specific information needed for a determination.
Most treating clinicians have never been trained to write in this functional language. The result is that many mental health disability files contain hundreds of pages of treatment notes that document genuine suffering and a valid diagnosis — but do not contain the specific functional evidence SSA needs to approve the claim.
2.4 The Structural Bias Problem
Research has documented significant structural inconsistency in how mental health claims are adjudicated. Dahl, Kostol, and Mogstad (2014) found that random assignment to different ALJs produced systematically different outcomes — whether a claim was approved depended in part on which judge heard it. Keiser (1999) documented state-level variation in implementation, meaning identical claimants received different determinations depending on where they lived. Deshpande and Li (2019) found that when SSA field offices closed, disability applications dropped 16% — not because fewer people were disabled, but because the administrative barrier was enough to screen out legitimately impaired applicants, particularly those with moderate-severity mental health conditions and lower education levels.
These findings point to a system where the quality of the evidence in the file — not just the severity of the condition — plays a decisive role in the outcome.
3. What SSA Actually Evaluates: The Five-Step Sequential Process
SSA uses a five-step sequential evaluation process for every disability claim. Understanding this process is essential because it reveals where in the decision-making chain mental health evidence has the greatest impact — and where it most commonly falls short.
Step 1: Substantial Gainful Activity (SGA)
The first question SSA asks is whether the claimant is currently engaged in substantial gainful activity — meaning work that earns above a threshold amount. In 2026, that threshold is $1,690 per month for non-blind claimants and $2,830 per month for blind claimants. If the claimant is working above SGA, the claim is denied regardless of the severity of their condition.
For many mental health claimants, this step is straightforward: they have already been unable to work for months or years before applying. But it is worth noting that some claimants attempt to continue working at reduced capacity — working part-time, accepting lower-level positions, or relying heavily on employer accommodations — and may be earning above SGA despite significant functional impairment. In these cases, careful documentation of the conditions under which work is maintained (and the unsustainability of those conditions) becomes important.
Step 2: Severity
The second question is whether the claimant's impairment "significantly limits" their ability to perform basic work activities. This is a threshold screening step with a relatively low bar. Most claimants with diagnosed mental health conditions and some documentation of functional limitation will pass Step 2. Claims that fail here typically have inadequate medical evidence of any kind — not a clinical deficiency, but a documentation deficiency.
Step 3: The Listing of Impairments (The Blue Book)
Step 3 is where the most consequential evaluation of mental health claims occurs. SSA maintains a "Listing of Impairments" — commonly called the Blue Book — that describes specific medical conditions and the criteria required to establish disability. If a claimant's condition meets or medically equals the criteria of a listing, they are found disabled without further analysis.
For mental health conditions, the relevant listings fall under Section 12.00 of the Blue Book. The most commonly invoked listings for mental health disability claims are:
Listing| Condition Category
12.02: Neurocognitive disorders
12.04: Depressive, bipolar, and related disorders
12.06: Anxiety and obsessive-compulsive disorders
12.07: Somatic symptom and related disorders
12.08: Personality and impulse-control disorders
12.15: Trauma- and stressor-related disorders
Each listing has two components. Paragraph A requires medical documentation of the diagnosis itself — clinical findings, signs, symptoms, and laboratory findings that establish the condition exists. Paragraph B evaluates the severity of the condition by measuring functional limitation across four specific areas.
The Paragraph B Criteria: The Four Functional Areas
The Paragraph B criteria are the heart of mental health disability evaluation. SSA rates the claimant's degree of limitation in four areas of mental functioning:
1. Understanding, remembering, or applying information. This area examines the ability to learn new things, remember and use information, follow instructions, solve problems, use judgment, and apply knowledge to new situations. Limitations in this area affect a worker's ability to understand procedures, remember work-like tasks, carry out instructions, and correct mistakes.
2. Interacting with others. This area examines the ability to relate to and work with supervisors, coworkers, and the public. It includes cooperative behaviors, handling conflicts, responding appropriately to social cues, maintaining socially appropriate behavior, and communicating clearly. Limitations in this area affect a worker's ability to function in a workplace that requires any interpersonal contact.
3. Concentrating, persisting, or maintaining pace. This area examines the ability to focus attention on work activities and to sustain that focus long enough to permit timely and appropriate completion of tasks. It includes the ability to work at a consistent pace, avoid distractions, complete a normal workday and workweek, and work without requiring an unreasonable number of rest periods. This is often the most critical area for mental health claims — sustained concentration over a full workday and workweek is precisely what many mental health conditions impair.
4. Adapting or managing oneself. This area examines the ability to regulate emotions, control behavior, maintain well-being, and respond to demands, changes, and stressors in work settings. It includes awareness of normal hazards, personal hygiene, maintaining appropriate behavior, and adapting to changes in routine.
SSA rates each of these four areas on a five-point scale:
Rating:
None: No limitation. Able to function independently, appropriately, effectively, and on a sustained basis.
Mild: Slightly limited but able to function well. Does not significantly affect the ability to work.
Moderate: Functioning is fair. The limitation exists but does not prevent all work-related activity.
Marked: Seriously limited. The ability to function independently, appropriately, effectively, and on a sustained basis is significantly reduced.
Extreme: Unable to function in this area independently, appropriately, effectively, and on a sustained basis.
To meet the Paragraph B criteria, a claimant must have either: an extreme limitation in one of the four areas, or marked limitations in two of the four areas.
This is the threshold where most mental health claims either succeed or fail. And it is the threshold where the quality of psychological evidence matters most. A consultative examination that rates a claimant's limitations as "moderate" across all four areas — when a comprehensive evaluation with standardized testing and longitudinal data would document "marked" limitations in two or more areas — is the difference between denial and approval.
The Paragraph C Alternative
For certain listings (12.02, 12.03, 12.04, 12.06, and 12.15), SSA offers an alternative to meeting Paragraph B. The Paragraph C criteria apply when a claimant has a serious and persistent mental disorder — documented over at least two years — and relies on ongoing medical treatment, therapy, psychosocial support, or a highly structured living environment to diminish symptoms, and has only marginal adjustment: minimal capacity to adapt to changes in environment or demands that are not already part of daily life.
Paragraph C captures claimants whose conditions appear "managed" only because they live within severely constrained circumstances. Remove the support structure, and functioning collapses. This pathway is particularly relevant for claimants with chronic depression, PTSD, or anxiety disorders who have been in continuous treatment for years but have never achieved the functional capacity for competitive employment.
Step 4: Residual Functional Capacity (RFC)
If a claimant's condition does not meet or equal a listing at Step 3, SSA proceeds to Step 4: assessing the claimant's Residual Functional Capacity (RFC). The RFC describes what the claimant can still do despite their limitations. For mental health claims, the RFC addresses the same four functional areas from Paragraph B but in more granular terms — specifying, for example, that the claimant can follow simple one- or two-step instructions but not complex multi-step procedures, or can work in proximity to coworkers but not in a position requiring frequent public contact.
The RFC assessment is where independent psychological evaluation evidence has its greatest practical impact. Many claimants whose conditions do not meet the rigid threshold of a listing (marked limitation in two areas) nonetheless have a combination of moderate and marked limitations that, taken together, preclude competitive employment. The RFC is the mechanism for capturing this nuance — but only if the file contains evidence specific enough for the adjudicator to build an accurate functional picture.
A treatment note that says "patient continues to struggle with depression" does not help with RFC. An independent evaluation report that says "the claimant is able to understand and remember simple, routine instructions but experiences significant difficulty with tasks requiring sustained concentration beyond 15-20 minutes, as evidenced by a Trails B completion time at the 3rd percentile and a WAIS-IV Processing Speed Index of 72" gives the adjudicator specific, testable data to work with.
Step 5: Adjustment to Other Work
If SSA determines at Step 4 that the claimant cannot perform their past relevant work, it proceeds to Step 5: whether the claimant can adjust to other work that exists in the national economy. SSA considers the claimant's RFC, age, education, and work experience. At ALJ hearings, a vocational expert typically testifies about what jobs exist for someone with the claimant's RFC profile.
This is another stage where the specificity of mental health evidence matters. An RFC that says "limited to simple, routine work" eliminates some jobs. An RFC that says "limited to simple, routine work, in a low-stress environment with minimal changes in routine, no public contact, no more than occasional contact with coworkers and supervisors, and a sit-stand option due to psychomotor agitation associated with anxiety" eliminates considerably more.
The detail in the RFC depends entirely on the detail in the medical evidence. Generic evidence produces generic RFCs. Specific evidence produces specific — and often more restrictive — RFCs.
4. The Consultative Examination Gap: Why SSA's Own Process Produces Incomplete Evidence
When SSA lacks sufficient medical evidence in the file to make a disability determination, it orders a consultative examination (CE). For mental health claims, this means a psychological evaluation conducted by a contracted examiner — a psychologist or, in some states, a licensed clinical social worker — who is paid by SSA to evaluate the claimant and write a report.
Consultative examinations serve an important function: they ensure that claimants who lack regular treatment providers still have their conditions professionally assessed. But the CE process has structural limitations that consistently produce evidence of lower quality and specificity than what the adjudicator needs for complex mental health claims.
4.1 Time Constraints
A typical psychological CE lasts 30 to 45 minutes. In that time, the examiner is expected to conduct a clinical interview, make behavioral observations, assess current mental status, and form diagnostic impressions. The entire evaluation — history, symptoms, mental status, diagnosis, and functional assessment — must be completed in a single session that is shorter than most therapy appointments.
For straightforward presentations — a claimant with a single, clearly documented condition and a consistent symptom picture — this may be sufficient. For the more common presentation — comorbid depression and anxiety, PTSD with substance use history, cognitive complaints layered over chronic pain — 40 minutes is not enough time to conduct the kind of thorough assessment that a complex case demands.
4.2 No Standardized Testing
Most CEs do not include formal psychological testing. The evaluation relies primarily on the clinical interview and mental status examination — both of which are clinician-dependent and produce subjective data. Standardized cognitive testing (IQ assessment, processing speed, memory testing), personality assessment, symptom validity measures, and structured diagnostic interviews are rarely part of the CE protocol.
This means the CE examiner is forming impressions about cognitive functioning, emotional regulation, and personality pathology based on a brief conversation rather than on normed, validated instruments that can be compared to population-level data. When a claimant reports difficulty concentrating, the CE examiner notes this in the report. An independent evaluator administers the Trail Making Test, the WAIS-IV, and the Conners CPT and documents how much difficulty exists, in what domains, and how it compares to age-matched norms.
4.3 No Effort or Validity Testing
Chafetz (2008) documented a significant structural problem in the CE process: SSA policy has historically discouraged CE examiners from incorporating formal effort and validity testing into their evaluations. Effort testing — measures such as the Test of Memory Malingering (TOMM) or the Word Memory Test (WMT) — assesses whether the claimant's test performance is consistent with genuine cognitive impairment or whether the claimant is exaggerating or fabricating symptoms.
This creates a paradox. SSA is concerned about the integrity of disability claims, yet the evaluation process it funds does not include the instruments specifically designed to assess that integrity. Independent evaluations routinely include effort and validity measures — not because the evaluator presumes the claimant is malingering, but because the absence of validity data weakens the credibility of the entire evaluation. When an independent report includes validity testing that confirms the claimant's presentation is credible and consistent, it gives the adjudicator a stronger evidentiary basis for the determination.
4.4 No Record Review, No Collateral Data
CE examiners typically do not have access to the claimant's treatment records during the examination. They are evaluating the claimant in isolation — without the context of treatment history, prior diagnoses, medication trials, hospitalization records, or third-party reports from family members or employers. The examiner is forming impressions about a chronic condition based entirely on what the claimant reports and how they present during a single brief encounter.
An independent evaluation, by contrast, begins with a comprehensive review of all available records. The evaluator reads the treatment history before ever meeting the claimant, identifies discrepancies and patterns in the longitudinal record, and uses the clinical interview to explore specific areas that the records flag. Collateral interviews with family members, former employers, or treating clinicians provide additional perspective on functional limitations that the claimant may underreport (due to poor insight) or overreport (due to distress).
4.5 The Structural Incentive Problem
CE examiners are paid a flat fee per evaluation — typically between $200 and $500, depending on the state. The economic incentive is to complete evaluations efficiently, not comprehensively. An examiner who spends three hours on a complex case and two hours writing a detailed report earns the same fee as one who completes the evaluation in 40 minutes and produces a two-page report. Over time, this incentive structure favors brevity.
Additionally, CE examiners are repeat contractors for SSA. While there is no evidence of systematic bias in CE findings, the structural relationship — the examiner is paid by the same agency that adjudicates the claim — creates at least the appearance of a conflict that an independent evaluator, retained by the claimant or claimant's attorney, avoids entirely.
5. What an Independent Psychological Evaluation Provides
An independent psychological evaluation is a comprehensive assessment conducted by a licensed psychologist who is not employed by or contracted with SSA. The evaluator is retained to conduct a thorough, objective evaluation of the claimant's psychological functioning and to produce a detailed report that addresses the specific functional questions relevant to disability determination.
The word "independent" is important. The evaluator is not an advocate for the claimant. The evaluator's obligation is to conduct an objective assessment and report the findings accurately — whether those findings support the claim or not. An evaluation that finds the claimant does not have disability-level functional impairment is just as valid and useful as one that does. The purpose is accuracy, not a predetermined conclusion.
5.1 Components of a Comprehensive Independent Evaluation
A quality independent psychological evaluation for disability determination typically includes the following components:
Comprehensive clinical interview (2-4 hours across one or more sessions). The interview covers psychiatric history, medical history, developmental history, educational and occupational history, social functioning, substance use history, current symptoms, daily activities, and functional capacity. Unlike a 40-minute CE, the extended clinical interview allows the evaluator to explore areas of complexity, follow up on inconsistencies, and develop a detailed picture of the claimant's psychological functioning in real-world contexts.
Standardized psychological testing. Depending on the clinical presentation, testing may include:
Cognitive assessment (e.g., WAIS-IV, WMS-IV, Trails A/B) to document intellectual functioning, processing speed, memory, and attention
Personality and emotional assessment (e.g., MMPI-3, PAI) to document psychological distress, personality pathology, and symptom patterns
Symptom-specific measures (e.g., PHQ-9 for depression, GAD-7 for anxiety, PCL-5 for PTSD) to quantify current symptom severity
Functional assessment measures to document limitations in activities of daily living and work-related activities
Effort and symptom validity testing (e.g., TOMM, SIMS, RDS) to establish the credibility and consistency of the claimant's presentation. Valid effort testing strengthens the report's findings by demonstrating that the claimant engaged authentically with the evaluation process.
Comprehensive record review. The evaluator reviews all available medical records, treatment notes, prior evaluations, hospitalization records, and other documentation before the clinical interview. This allows the evaluator to identify patterns in the longitudinal record, corroborate self-reported history, and note discrepancies that require clinical exploration.
Collateral information. When appropriate, the evaluator contacts family members, former employers, treating clinicians, or other individuals who can provide perspective on the claimant's functioning in contexts the claimant may not accurately report — either because of poor self-awareness, cognitive impairment, or the nature of the condition itself (e.g., a claimant with anosognosia secondary to brain injury may genuinely not recognize the severity of their cognitive deficits).
5.2 How Independent Evaluations Address the Paragraph B and RFC Gap
The central value of an independent evaluation is that it produces evidence specifically calibrated to the questions SSA needs answered. Rather than describing symptoms in general clinical language, the evaluation report maps findings directly to the four Paragraph B functional areas and articulates the specific ways the claimant's conditions limit work-related functioning.
For example, rather than stating that the claimant "has difficulty with concentration," an independent evaluation might document:
On formal cognitive testing, the claimant's WAIS-IV Processing Speed Index score of 74 (4th percentile) and Working Memory Index score of 78 (7th percentile) indicate significant impairment in sustained attention and the ability to hold and manipulate information — capacities essential to maintaining pace in a competitive work environment. These findings are consistent with the claimant's self-report of an inability to read more than a few pages without losing the thread, and with her spouse's report that the claimant routinely abandons household tasks midstream and requires repeated reminders to complete basic responsibilities. On the Trail Making Test Part B, the claimant's completion time of 156 seconds (3rd percentile for age) reflects difficulty with cognitive flexibility and divided attention that would significantly impair performance on tasks requiring attention to multiple demands. These findings support a rating of marked limitation in the area of concentrating, persisting, or maintaining pace.
This level of specificity — testing data, behavioral observations, collateral reports, and a direct mapping to SSA's functional categories — is what the adjudicator needs and what the CE process rarely provides.
5.3 Documenting Comorbidity and Interactive Effects
Many claimants with mental health conditions have more than one diagnosis. Depression commonly co-occurs with anxiety. PTSD frequently co-occurs with substance use disorders. Cognitive impairment may coexist with mood disturbance. These comorbid conditions interact to produce functional impairment greater than what any single diagnosis alone would suggest.
Independent evaluations document these interactive effects systematically. For example, an evaluation might explain that the claimant's depressive disorder impairs motivation and energy, their anxiety disorder impairs concentration and tolerance for workplace stress, and their chronic insomnia impairs cognitive processing speed — and that the combination of these three conditions produces marked limitations in concentrating, persisting, and maintaining pace and in adapting and managing oneself, even though each condition individually might produce only moderate limitation.
This interaction analysis is essential because SSA evaluates the combined impact of all conditions, not each condition in isolation. But the evidence in the file must explicitly describe the interactions. An adjudicator reviewing three separate treatment notes from three separate providers — a psychiatrist managing medication, a therapist documenting therapy sessions, and a primary care physician noting sleep complaints — may not synthesize the interaction pattern. An independent evaluation that reviews all three sets of records and integrates them into a unified functional assessment does this synthesis for the adjudicator.
6. Where Independent Evidence Fits in the SSDI Process
Independent psychological evaluations can be submitted at any stage of the SSDI process. The strategic timing depends on the specific circumstances of the claim.
6.1 Initial Application
Submitting independent evaluation evidence with the initial application produces the strongest evidentiary foundation. Many initial denials result from insufficient evidence — the file contains only treating clinician notes that describe symptoms without functional language, or the only psychological evidence is a brief CE. An independent evaluation submitted at the initial stage gives the Disability Determination Services (DDS) examiner detailed, specific functional evidence from the outset.
For claimants who do not have a treating mental health provider — or whose treating provider's documentation does not address functional limitations — an independent evaluation may be the only comprehensive psychological evidence in the file.
6.2 Reconsideration
If the initial application is denied, the first level of appeal is reconsideration. At this stage, a different DDS examiner reviews the file and any new evidence. Submitting an independent evaluation at reconsideration addresses whatever evidentiary deficiency led to the initial denial. If the denial letter identifies specific reasons (e.g., "the evidence does not establish marked limitation in any area of mental functioning"), the independent evaluation can directly address those reasons with testing data and detailed functional analysis.
6.3 ALJ Hearing
The ALJ hearing is where independent psychological evaluation evidence has its greatest impact. Unlike the DDS stage — where decisions are made by examiners reviewing paper files — the ALJ hearing is an in-person or video proceeding where the judge can review all evidence, question the claimant, consult a vocational expert, and exercise considerable discretion in weighing competing evidence.
When an independent evaluation report is in the file, the ALJ has several pieces of evidence that a typical file lacks:
Standardized testing data that quantifies functional limitations
Effort/validity testing that addresses the credibility of the claimant's presentation
A longitudinal analysis based on comprehensive record review
A professional opinion, supported by data, that directly addresses the Paragraph B criteria and RFC
Collateral data from sources beyond the claimant's self-report
ALJs are required to consider and address evidence from acceptable medical sources — and licensed psychologists are explicitly designated as acceptable medical sources under SSA regulations (20 CFR 404.1502). The ALJ cannot simply disregard an independent evaluation; if the ALJ disagrees with its conclusions, the ALJ must explain why, providing the claimant's attorney an opportunity to address any concerns.
7. Qualifications of an Independent Evaluator: What Claimants and Attorneys Should Look For
Not all psychological evaluations are created equal. The quality, methodology, and credibility of an independent evaluation depend on the qualifications of the evaluator and the rigor of their assessment process. Claimants and attorneys selecting an independent evaluator should consider the following factors.
7.1 Licensure and Credentials
The evaluator must be a licensed psychologist — Ph.D. or Psy.D. — practicing at the independent level. Under SSA regulations, licensed psychologists are "acceptable medical sources" whose evaluations can establish a medically determinable impairment. Licensed clinical social workers, licensed professional counselors, and other mental health professionals can provide supporting evidence but cannot establish a medically determinable impairment on their own.
7.2 Forensic Evaluation Training
There is a fundamental difference between clinical psychology (therapy, treatment) and forensic psychology (objective evaluation for legal and administrative proceedings). As Strasburger, Gutheil, and Brodsky (1997) established in their landmark paper "On Wearing Two Hats," the treating clinician role and the forensic evaluator role are structurally incompatible. A treating therapist advocates for the patient's wellbeing. A forensic evaluator advocates for the accuracy of the findings — regardless of whether those findings favor the examinee.
The evaluator conducting an independent disability evaluation should have training and experience in forensic assessment methodology, including:
Administration and interpretation of standardized psychological testing
Effort and symptom validity assessment
Structured diagnostic interviewing
Integration of multi-source data (records, testing, collateral) into a coherent clinical formulation
Understanding of the legal and administrative framework in which the evaluation will be used
7.3 Familiarity with SSA's Framework
An evaluator who understands SSA's five-step process, the Paragraph B criteria, and the RFC assessment can write a report that speaks the adjudicator's language. An evaluator who writes a standard clinical report — diagnosis, symptoms, treatment recommendations — produces a document that may be clinically valid but does not address the functional questions SSA needs answered.
The best independent evaluations are written by psychologists who understand that the purpose of the report is not to diagnose (though diagnosis is part of it) but to document how the diagnosed condition affects the claimant's ability to perform sustained competitive employment. This requires a different lens than clinical practice.
7.4 Methodology Markers of a Quality Evaluation
Claimants and attorneys should expect the following from a quality independent evaluation:
Comprehensive clinical interview of sufficient length and depth to explore the full clinical picture — not a 30-minute screening
Standardized psychological testing with normed instruments selected for the clinical questions at hand
Effort and validity testing — its presence strengthens the report; its absence raises questions about the rigor of the evaluation
Comprehensive record review integrated into the report's findings and conclusions
A report that maps findings to SSA's specific functional criteria — Paragraph B areas, RFC limitations, or both
A clear distinction between clinical data and clinical opinion — the adjudicator needs to see what the data shows and what the evaluator concludes from it, separately
7.5 Red Flags
An evaluator who guarantees a favorable outcome. No ethical evaluator can promise that an evaluation will result in approval of benefits. The evaluation documents functional status accurately — the outcome depends on many factors beyond the evaluation itself.
No psychological testing. An "evaluation" that consists only of an interview and a letter does not meet the standard of a comprehensive independent evaluation.
A report that reads like advocacy. The report should document findings objectively. If the report reads like a brief arguing for approval, it will be received with skepticism by the adjudicator — and rightly so.
A report that does not address SSA's functional criteria. If the report describes symptoms and diagnoses but does not address the four Paragraph B areas or articulate specific functional limitations, it does not fill the evidentiary gap that independent evaluations are meant to address.
An extremely brief report. Complex mental health presentations produce complex functional pictures. A two- or three-page report is unlikely to capture the nuance that disability determination requires.
8. The Mental Health Conditions Most Commonly at Issue in Disability Claims
This section describes the mental health conditions most frequently involved in SSDI claims, the Blue Book listings under which they are evaluated, and the common evidentiary gaps that lead to denials.
8.1 Major Depressive Disorder (Listing 12.04)
Major depressive disorder (MDD) is one of the most common primary diagnoses in mental health disability claims. The challenge with MDD claims is not typically diagnosis — the condition is well-documented in most treatment records. The challenge is severity documentation. Treating clinicians describe depressive symptoms (low mood, sleep disruption, appetite changes, anhedonia) but often do not quantify the functional impact of those symptoms.
An independent evaluation for MDD typically includes objective measures of depression severity (e.g., BDI-II, PHQ-9), cognitive testing to document the concentration and processing speed deficits that depression commonly produces, and a functional analysis that connects documented symptoms to specific Paragraph B limitations.
8.2 Generalized Anxiety Disorder (Listing 12.06)
GAD presents a particular challenge for disability evaluation because anxiety symptoms are often invisible in structured, low-demand settings — like a 40-minute consultative exam. A claimant with severe GAD may present as pleasant, articulate, and cooperative during the CE because the examination setting is one-on-one, predictable, and low-stakes. The same claimant may decompensate under the sustained interpersonal demands, unpredictable stressors, and performance expectations of competitive employment.
Independent evaluations document this discrepancy by assessing anxiety across contexts — work history, daily activities, interpersonal functioning — and by using standardized anxiety measures and cognitive testing to capture the attentional and processing deficits that chronic anxiety produces.
8.3 Post-Traumatic Stress Disorder (Listing 12.15)
PTSD is uniquely self-undermining in the disability process. The avoidance symptoms that are central to the diagnosis — avoiding reminders of trauma, avoiding stressful situations, withdrawing from social engagement — are the same symptoms that prevent claimants from attending appointments, engaging fully with evaluators, and providing the detailed, consistent self-report that the evaluation process demands. A claimant who minimizes symptoms during a brief CE because full disclosure feels too threatening may be mistakenly assessed as having only moderate limitations.
Independent evaluations account for this by building rapport over extended sessions, using structured diagnostic interviews (e.g., the Clinician-Administered PTSD Scale, CAPS-5), and contextualizing avoidance behavior as a symptom — not as evidence that the condition is less severe than claimed.
8.4 Bipolar Disorders (Listing 12.04)
The episodic nature of bipolar disorders means that a single-point-in-time evaluation can dramatically misrepresent functional capacity. A claimant evaluated during a euthymic or mildly hypomanic period may appear entirely functional. The same claimant evaluated during a depressive episode may present as severely impaired. Neither snapshot captures the pattern of cycling between states that is the hallmark of the disorder and the primary source of functional impairment.
Independent evaluations address this by reviewing longitudinal treatment records for documentation of cycling patterns, assessing the frequency and severity of episodes over time, and documenting the cumulative functional impact — not just the current-state presentation.
8.5 Cognitive Impairment and Neurocognitive Disorders (Listing 12.02)
Claims involving cognitive impairment — whether from traumatic brain injury, neurodegenerative disease, chronic substance use, or other causes — almost always require formal neuropsychological testing that CEs do not include. Without standardized cognitive testing, claims of difficulty with memory, concentration, processing speed, or executive functioning rest entirely on self-report and clinical observation. Testing data — IQ scores, memory indices, processing speed indices, executive function measures — provides the objective, normed evidence that adjudicators need.
8.6 Comorbid Presentations
As noted in Section 5.3, comorbidity is the rule rather than the exception in disability-level mental health impairment. A claimant with MDD alone may have moderate limitations. The same claimant with MDD, GAD, chronic insomnia, and chronic pain may have marked limitations in two or more Paragraph B areas due to the interactive effects of multiple conditions.
Independent evaluations are particularly valuable for comorbid presentations because they assess all conditions in a single evaluation and explicitly document the interactions — something that treatment notes from multiple separate providers rarely do.
9. The Broader Context: Why Mental Health Disability Claims Are Rising
Mental health disability claims have been increasing for decades, and the forces driving this trend are not slowing down. Understanding the broader context helps explain why the need for quality mental health evidence in SSDI cases is growing, not shrinking.
9.1 SSDI as a De Facto Safety Net
Autor and Duggan (2006) described SSDI as a program that has historically absorbed displaced workers from declining industries. When trade competition devastated American manufacturing in the 1990s and 2000s, displaced workers in affected communities did not simply transition to new careers. Many left the labor force entirely — and a significant number applied for and received disability benefits. Autor, Dorn, Hanson, and Song (2014) documented this pathway empirically: workers displaced by trade competition had elevated rates of SSDI receipt. Displacement led to disability, not because the workers were physically different from their peers, but because prolonged unemployment, loss of identity, and deteriorating mental and physical health produced disability-level impairment over time.
This pattern — economic displacement cascading into psychological deterioration and then disability — is likely to recur as artificial intelligence and automation reshape the labor market. The populations most at risk may be different (knowledge workers, professionals, and college-educated entry-level workers rather than manufacturing workers), but the biopsychosocial pathway from displacement to disability is well-established in the research literature (Paul & Moser, 2009; Stuckler et al., 2009; Case & Deaton, 2015).
9.2 The Staffing Crisis
The SSDI system is under significant operational strain. Between January 2025 and January 2026, SSA lost approximately 7,500 employees — 13% of its total workforce — and 13% of its Administrative Law Judges, the fewest in at least 20 years. Pending hearing backlogs rose by approximately 73,000 cases during this period, and some Disability Determination Services offices are operating at less than 30% staffing with active hiring freezes in place.
For claimants with mental health conditions, the operational strain compounds the evidentiary problem. Longer wait times mean longer periods of unemployment, financial deterioration, and psychological decline before a hearing. Understaffed DDS offices reviewing files quickly may be less likely to engage deeply with nuanced mental health evidence. The quality of the evidence in the file becomes even more critical when the adjudicator has less time to spend with each case.
9.3 The Absence of Structural Alternatives
Hoynes and Rothstein (2019) observed that Universal Basic Income would fill many of the gaps that SSDI currently cannot — providing income support to displaced workers without requiring them to demonstrate disability. Moffitt (2015) documented that welfare spending has shifted toward disability programs and away from direct assistance to non-disabled working-age adults, making SSDI a broader safety net than it was originally designed to be.
In the absence of UBI or comparable structural reform — robust retraining programs, employer-funded transition support, portable health insurance — SSDI is one of the few mechanisms available to American families when a worker develops disability-level impairment from any cause, including the psychological consequences of workforce displacement. This does not mean SSDI is the right solution to the problem of AI displacement. It means SSDI is, for many families, the only solution currently available.
10. Conclusion: Bridging the Gap Between Impairment and Recognition
Mental health conditions produce real, measurable, disability-level functional impairment that prevents millions of Americans from engaging in sustained competitive employment. The research on this point is not ambiguous: across hundreds of studies and hundreds of thousands of participants, involuntary job loss, chronic unemployment, and the psychiatric conditions they produce or exacerbate consistently impair functioning across cognitive, emotional, interpersonal, and adaptive domains (Paul & Moser, 2009; McKee-Ryan et al., 2005; Gedikli et al., 2022).
SSA's disability determination process is designed to evaluate this impairment. But SSA's own evidence-gathering mechanisms — particularly the consultative examination — are structurally limited in ways that systematically disadvantage mental health claimants. The CE is too brief, lacks standardized testing, omits validity assessment, and evaluates claimants without the benefit of longitudinal records or collateral data. The result is that many legitimately impaired claimants are denied benefits not because they are not disabled, but because the evidence in the file does not adequately document the severity and functional impact of their conditions.
Independent psychological evaluations conducted by qualified forensic psychologists address this evidentiary gap. They provide the comprehensive clinical interview, the standardized testing data, the effort and validity assessment, the longitudinal record review, the collateral information, and the functional analysis — all mapped to the specific criteria SSA uses to make determinations — that the CE process does not reliably produce.
This is not about gaming the system. It is about ensuring the system has the information it needs to reach an accurate determination. An independent evaluation that finds the claimant is not disabled is just as valuable as one that finds they are — because in either case, the determination rests on complete evidence rather than incomplete evidence.
For claimants navigating the SSDI process with mental health conditions, for the attorneys who represent them, and for the clinicians who treat them: the quality of psychological evidence is not a marginal factor in disability determination. It is often the deciding factor. Understanding what that evidence should contain, who is qualified to produce it, and where it fits in the adjudication process is essential for ensuring that the system works as it was designed to — not as a barrier to benefits, but as a mechanism for accurately identifying who needs them.
References
Anfang, S. A., Gold, L. H., & Meyer, D. J. (2019). AAPL practice resource for the forensic evaluation of psychiatric disability. Journal of the American Academy of Psychiatry and the Law, 47(Suppl 5), S1-S51.
Autor, D. H. (2015). Why are there still so many jobs? The history and future of workplace automation. Journal of Economic Perspectives, 29(3), 3-30.
Autor, D. H., & Duggan, M. G. (2003). The rise in the disability rolls and the decline in unemployment. The Quarterly Journal of Economics, 118(1), 157-206.
Autor, D. H., & Duggan, M. G. (2006). The growth in the Social Security disability rolls: A fiscal crisis unfolding. Journal of Economic Perspectives, 20(3), 71-96.
Autor, D. H., Dorn, D., & Hanson, G. H. (2013). The China Syndrome: Local labor market effects of import competition in the United States. American Economic Review, 103(6), 2121-2168.
Autor, D. H., Dorn, D., Hanson, G. H., & Song, J. (2014). Trade adjustment: Worker-level evidence. The Quarterly Journal of Economics, 129(4), 1799-1860.
Bound, J. (1989). The health and earnings of rejected disability insurance applicants. The American Economic Review, 79(3), 482-503.
Case, A., & Deaton, A. (2015). Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century. Proceedings of the National Academy of Sciences, 112(49), 15078-15083.
Chafetz, M. D. (2008). Malingering on the Social Security Disability Consultative Exam: Predictors and base rates. The Clinical Neuropsychologist, 22(3), 529-546.
Chafetz, M. D. (2011). The psychological consultative examination for Social Security Disability. Psychological Injury and Law, 4(3-4), 235-244.
Christensen, J., Aarøe, L., Baekgaard, M., Herd, P., & Moynihan, D. P. (2020). Human capital and administrative burden: The role of cognitive resources in citizen-state interactions. Public Administration Review, 80(1), 127-136.
Dahl, G. B., Kostøl, A. R., & Mogstad, M. (2014). Family welfare cultures. The Quarterly Journal of Economics, 129(4), 1711-1752.
Deshpande, M., & Li, Y. (2019). Who is screened out? Application costs and the targeting of disability programs. American Economic Journal: Economic Policy, 11(4), 213-248.
Gedikli, C., Miraglia, M., Connolly, S., Bryan, M., & Watson, D. (2022). The relationship between unemployment and wellbeing: An updated meta-analysis of longitudinal evidence. European Journal of Work and Organizational Psychology, 32(1), 1-17.
Hoynes, H. W., & Rothstein, J. (2019). Universal basic income in the United States and advanced countries. Annual Review of Economics, 11, 929-958.
Keiser, L. R. (1999). State bureaucratic discretion and the administration of Social Security Disability Insurance. Journal of Public Administration Research and Theory, 9(1), 87-106.
McKee-Ryan, F. M., Song, Z., Wanberg, C. R., & Kinicki, A. J. (2005). Psychological and physical well-being during unemployment: A meta-analytic study. Journal of Applied Psychology, 90(1), 53-76.
Moffitt, R. A. (2015). The deserving poor, the family, and the U.S. welfare system. Demography, 52(3), 729-749.
Neal, T. M. S., & Grisso, T. (2014). Assessment practices and expert judgment methods in forensic psychology and psychiatry: An international snapshot. Criminal Justice and Behavior, 41(12), 1406-1421.
Paul, K. I., & Moser, K. (2009). Unemployment impairs mental health: Meta-analyses. Journal of Vocational Behavior, 74(3), 264-282.
Steenbeek, R., Schellart, A. J. M., Mulders, H., Anema, J. R., Kroneman, H., & Besseling, J. (2011). The development of instruments to measure the work disability assessment behaviour of insurance physicians. BMC Public Health, 11, 1-12.
Strasburger, L. H., Gutheil, T. G., & Brodsky, A. (1997). On wearing two hats: Role conflict in serving as both psychotherapist and expert witness. American Journal of Psychiatry, 154(4), 448-456.
Stuckler, D., Basu, S., Suhrcke, M., Coutts, A., & McKee, M. (2009). The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. The Lancet, 374(9686), 315-323.
About the Authors
Lisa A. Long, Psy.D. is a licensed clinical and forensic psychologist and the Clinical Director of Dr. Long & Associates, a national telehealth psychology practice specializing in forensic, immigration, and clinical psychological evaluations. Dr. Long is authorized to practice across 43 states through the Psychology Interjurisdictional Compact (PSYPACT) and has conducted over 500 forensic evaluations. She holds expertise in disability evaluation, parental capacity assessment, and clinical diagnostic assessment.
Leesandra Contreras-Gonzalez, Psy.D. is a licensed clinical psychologist at Dr. Long & Associates specializing in bilingual (English/Spanish) psychological evaluations. Dr. Contreras-Gonzalez brings expertise in culturally responsive assessment and serves populations with limited English proficiency — a critical capability given the demographic composition of the disability claimant population.
Disclaimer
This article is provided for informational and educational purposes only. It does not constitute legal advice, medical advice, or a guarantee of any particular outcome in a disability claim. Every disability case is unique, and outcomes depend on the specific facts, evidence, and circumstances of the individual claim. Dr. Long & Associates conducts independent psychological evaluations objectively — evaluation findings are reported accurately regardless of whether they support or do not support a disability claim. Individuals seeking guidance on their SSDI claim should consult with a qualified disability attorney
Published at drlisalong.com | Dr. Long & Associates | Nationwide Telehealth Psychological Evaluations|Contact Us